Pulmonary artery pseudoaneurysm
CASE REPORT AND LITERATURE REVIEW

Summary
Pseudoaneurysms of peripheral pulmonary arteries are a rare condition that can be linked to various causes and are associated with rupture and hemoptysis, with high mortality rates. One of the described causes, although infrequent, is the use of a Swan-Ganz catheter. We report the case of a patient who, during her hospitalization in the immediate postoperative period, presented with an episode of hemoptysis. Suspecting pulmonary thromboembolism (PTE), a computed tomography scan was performed, which detected a pseudoaneurysm of the anterior basal branch of the right pulmonary artery. After ruling out other causes, it was attributed to a complication of the Swan-Ganz catheter used during surgery. The patient underwent digital subtraction angiography to confirm the diagnosis and was treated with coil placement.
Keywords: pseudoaneurysm, hemoptysis, Swan-Ganz catheter, computed tomography.
Introduction
Pulmonary arterial balloon catheters, introduced in 1970 by Swan et al. (1), have been used as a method of hemodynamic monitoring in critically ill patients. Although it is usually a safe procedure, a variety of complications have been reported (2) , including the formation of pseudoaneurysms.
The aim of this presentation is to illustrate one of the complications of Swan-Ganz catheter use, which, although infrequent, should be considered when evaluating potential causes of hemoptysis in patients who have or have recently had a catheter. The use of multidetector computed tomography angiography (MDCT angiography), with a pulmonary artery opacification protocol, allows us to make this diagnosis with certainty, ruling out other causes (pulmonary embolism, pulmonary hemorrhage, etc.). Arriving at a precise diagnosis allows for treatment via catheterization, with embolization of the pseudoaneurysm.
Case presentation
An 80-year-old female patient presented for a total hip replacement due to a history of femoral neck fracture. During the immediate postoperative period, she experienced an episode of hemoptysis, without dyspnea or hemodynamic instability. Her only relevant medical history was the placement of a Swan-Ganz catheter during surgery, which was necessary given her cardiovascular status (heart failure with severe left ventricular dysfunction, mitral regurgitation, and aortic stenosis). Based on the clinical presentation and her medical history, pulmonary embolism was suspected. A lower extremity Doppler ultrasound was performed, which was negative, and a chest X-ray revealed a right paracardiac opacity. It is then decided to perform an MDCT Angio, which is carried out on a 64-row detector equipment, administering intravenous contrast at a rate of 4 ml/sec, with a protocol for visualization of pulmonary arteries using automatic triggering and with a threshold of 200 Hounsfield Units.
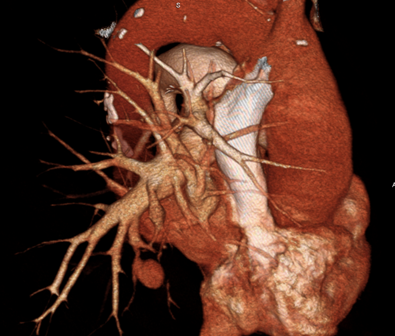
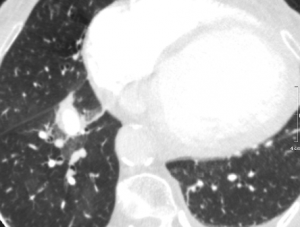
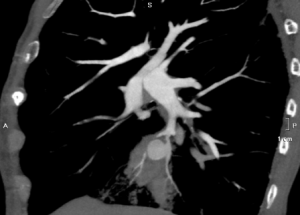
The examination did not demonstrate the presence of pulmonary embolism (PE), but it did reveal a ground-glass opacity with indistinct borders consistent with alveolar hemorrhage associated with another rounded image in close contact with the anterior basal branch of the right pulmonary artery, with the same density as the pulmonary vascular pool. Multiplanar, maximum intensity projection (MIP), and three-dimensional reconstructions were performed. Considering the recent history of pulmonary catheterization, a diagnosis of pseudoaneurysm of the aforementioned arterial branch was reached, probably as a complication of Swan-Ganz catheter placement.
A digital pulmonary artery angiography was then performed, which confirmed the presence of the pseudoaneurysm of the anterobasal artery of the right lower lobe and its embolization with fiber coils was performed and subsequent angiographic control which demonstrates total exclusion of the aneurysm.
The patient recovered without complications after the last procedure and was discharged in good general condition.

Discussion
Since its introduction in 1970, the Swan-Ganz catheter has been widely used, becoming an indispensable part of critical care and surgical management (3) . Multiple complications have been observed, the most frequent being arrhythmias, occurring in approximately 69% of patients (2) . Other complications are divided into those related to catheter insertion through a vascular access site (arterial laceration, pneumothorax, phrenic nerve injury, air embolism, etc.) and those related to the catheter itself (infection, valvular damage, thrombosis, pulmonary infarction, etc.) (3) . Pulmonary artery rupture occurs in 0.001 to 0.47% of cases, with an estimated mortality rate between 45% and 65%. In these cases, death occurs due to massive hemoptysis (4) . In a prospective study of 500 catheterized patients, complications were observed in 126 cases, of which only 23 (4.4%) were serious. Of these serious complications, only 8 were associated with massive hemoptysis and pulmonary infiltrates on chest X-ray (5) , highlighting the low frequency of this complication.
Several predisposing factors exist for vascular rupture, including anticoagulation, pulmonary hypertension, prolonged corticosteroid treatment, hypothermia during surgery, intraoperative cardiac manipulation, age over 60, and female sex (2-3-4) . The proposed injury mechanisms associated with the use of arterial catheters are varied. These include: an increase in intra-balloon pressure that exceeds the distensibility of the vascular wall and vascular perforation induced directly by the catheter tip against the vessel wall, which is more frequent in small-caliber vessels (3) . Regardless of the mechanism, pseudoaneurysm formation after catheter insertion has been described as an extremely rare complication in the cited articles.
Other causes of pulmonary artery rupture and pseudoaneurysm include tuberculosis (the so-called Rasmussen pseudoaneurysm), mycetomas, sarcoidosis, and several predisposing conditions such as cystic fibrosis, pulmonary hypertension, and arteriovenous malformations (6) . It is important to note that patients with tuberculosis have a higher risk of developing pseudoaneurysms than the general population (6) . Traumatic aneurysm not associated with Swan-Ganz is another cause to consider, although it is infrequent, with only 12 cases reported in the literature (7) .
The typical clinical presentation of this pathology is hemoptysis, followed by the appearance of an infiltrate with poorly defined margins on the chest X-ray, initially indistinguishable from a pulmonary infarction (8) , with a persistent denser central area corresponding to the pseudoaneurysm itself (3) . This infiltrate, with more defined borders, surrounds the pulmonary artery branch that contained the catheter and has been visualized up to seven months after the hemoptysis episode (8) . Typically, the condition presents within 24 hours of catheterization, although there are isolated cases in which it presents between 2 and 14 days later (2) . The right pulmonary artery is the most frequent location, occurring in 93% of cases, usually in the middle and lower lobes (3) .
The next proposed diagnostic step is CT angiography with pulmonary artery opacification protocol (3) , since it not only allows the recognition of a pseudoaneurysm but also the exclusion of other possible causes of hemoptysis (9-10) already mentioned and the planning of embolization (9) .
Although this pathology, as already mentioned, presents a high mortality rate, close to 70%, catheter embolization has become the treatment of choice, leading to a decrease in morbidity and mortality while confirming the diagnosis (3) and displacing the other therapeutic option, previously used, which was pulmonary resection (lobectomy) (4-11) . Angiography is the reference method in the diagnosis of pseudoaneurysms (3) and allows the placement of coils within the lumen of the aneurysmal sac, excluding it from the circulation (4-6) .
Conclusion
The use of Swan-Ganz catheters has become an indispensable tool for managing critically ill patients and during surgery. Rupture of a peripheral pulmonary artery with the formation of a pseudoaneurysm is a rare but potentially fatal complication. CT pulmonary angiography (CPA) allows for its accurate diagnosis and facilitates subsequent pulmonary angiography with coil embolization, which has become the treatment of choice. Early diagnosis using CPA in a patient who has had a catheter inserted and is experiencing hemoptysis is essential for a favorable outcome in this condition.
Literature
1- Swan H, Ganz W, Forrester J, Marcus H, Diamond G, Chonette D. Catheterization of the heart in man using a flow directed balloon tipped catheter. New England Journal of Medicine 1970; 283:447–451.
2- Dieden J, Friloux L, Renner J. Pulmonary artery false aneurysms secondary to Swan Ganz pulmonary artery catheters, AJR 1987; 149: 901-906.
3- Poplausky M, Rozemblit G, Rundback J, Crea G, Maddineni S, Leonardo R. Swan Ganz catheter-induced pulmonary artery pseudoaneurysm formation: the case reports and a review of the literature, Chest 2001; 120: 2105-2111.
4- Ferretti G, Thony F, Link K, Durand M, Wollschlager K, Blin D, et al. False aneurysm of the pulmonary artery induced by Swan Ganz catheter: clinical presentation and radiologic management, AJR 1996; 167: 941-945.
5- Boyd K, Thomas S, Gold J, Boyd A. A prospective study of the complications of pulmonary catheterizations in 500 consecutive patients, Chest 1983; 84: 245-249.
6- Sbano H, Mitchel A, Ind P, Jackson J. Peripheral pulmonary artery pseudoaneurysms and massive hemoptysis, AJR 2005; 184:1253-1259.
7- Savage C, Zwischenberger J, Ventura K, Wittich G. Hemoptysis secondary to pulmonary pseudoaneurysm 30 years after gunshot wound, The annals of thoracic surgery 2001; 71: 1021-1023.
8- Davis S, Neithamer C, Schreiber T, Sos T. False pulmonary artery aneurysm induced by Swan Ganz catheter: diagnosis and embolotherapy, Radiology 1987; 164: 741-742.
9- Bruzzi J, Rémy Jardin M, Delhaye D, Teisseire A, Khalil C, Rémy J. Multi-detector row CT of hemoptysis, Radiographics 2006; 26:3-22.
10- Khalil A, Fartoukh M, Tassart M, Parrot A, Marsault C, Carette M. Role of MDCT in identification of the bleeding site and the vessels causing hemoptysis, AJR 2007; 188: W117-W125.
11- Block M, Lefkowitz T, Ravenel J, Leon S, Hannegan C. Endovascular coil embolization for acute management of traumatic pulmonary artery pseudoaneurysm, Journal of thoracic and cardiovascular surgery 2004; 128: 784-785.
For any comments or suggestions: radiologyzones@gmail.com
This material was automatically translated from medicosradiologos.com.ar