Bone marrow edema
Based on the following case, we will analyze the possible causes of bone edema, its history, clinical presentation, and treatments.
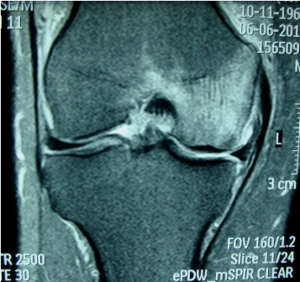
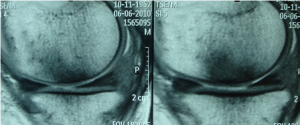
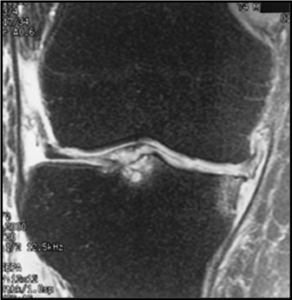
Case : 44-year-old patient, unilateral knee pain of 3 weeks’ duration. Denies trauma.
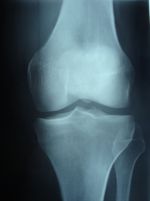
Based on these images, we propose the following differential diagnoses, which we will then analyze one by one.
- Bone contusion.
- Stress fracture.
- Osteonecrosis.
- Reactive changes to underlying degenerative joint disease.
- Transient bone marrow edema syndrome.
1- Transient bone marrow edema syndrome
- Male, between 30 and 60 years old.
- A joint condition that primarily affects the hip and less frequently the knee and ankle.
- There is usually a history of trauma (athletes).
- Pain and limited joint function, which may be accompanied by swelling of the soft tissues.
- Diagnosis confirmed by MRI.
- Negative X-rays and CT scans.
- Treatment:
Initial rest, ambulation with offloading, analgesics/NSAIDs, kinesitherapy.Good evolution, spontaneous resolution in 6 months.Be alert to rule out that the condition may be an initial phase of an avascular process.
2-Osteonecrosis
- Over 60 years old.
- M/F ratio 3:1.
- Sudden and severe unilateral pain (the patient remembers when or what they were doing).
- It does not calm with rest.
- It mainly affects the medial femoral condyle.
- Most cases are of unknown etiology. However, there are associated conditions, such as those listed below: Obesity, Sickle Cell Anemia, Thalassemia, Lupus, Kidney Transplant/Dialysis, HIV, Fatty Storage Disorders (Gaucher), Corticosteroids.
- Treatment :
-
Conservative: rest, physiotherapy and NSAIDs.
-
Surgical: core decompression for reduction of intraosseous pressure (restoring adequate circulation) and knee arthroplasty in advanced stages.
The following is an example of osteonecrosis of the femoral condyle in which edema in the bone marrow and a subchondral area of low signal, probably linked to subchondral microfracture (initial stage) are observed.
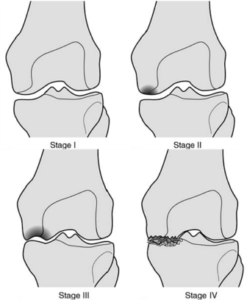
The following graph shows the evolution of an injury towards osteonecrosis.
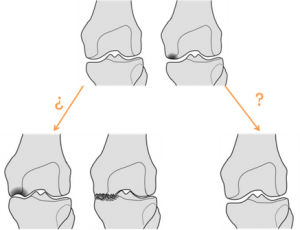
The following graph shows the indistinct possibility of the initial stages evolving towards osteonecrosis or towards resolution of the edema, making the time of evolution a determining factor.
3-Contusive edema (patterns)
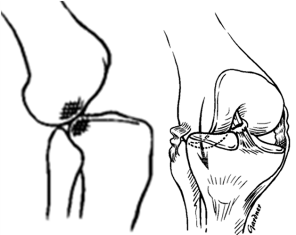
Pivot Shift Injury
- Knee flexed, femur internally rotated, valgus forced.
- Edema is classically found in the external condyle and posterior sector of the tibial plateaus.
- Associated injuries: anterior cruciate ligament rupture, medial collateral ligament injury, posterior horn injury of the medial or lateral meniscus.

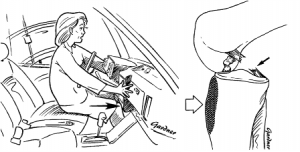
Dashboard injury
- The knee hits the dashboard of the car.
- The knee is flexed, with a tight posterior cruciate ligament.
- The tibia is forced posteriorly.
- There is edema in the bone marrow on the anterior aspect of the proximal tibia.
- Associated injuries: LCP.
Hyperextension injury
- Indirect force.
- Direct force.
- «Kissing» pattern. Bone marrow edema on the anterior aspect of the proximal tibia and distal femur.
- Associated injuries: ACL, PCL, Menisci.

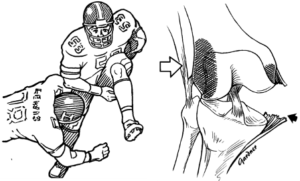
Clip-type injury
- Knee flexed and forced into valgus.
- Extensive bone marrow edema of the lateral femoral condyle (direct impact) and lesser edema in the medial condyle due to avulsion injury of the MCL (due to valgus stress).
- Associated injuries: MCL, ACL and menisci (O’Donoghue’s Triad).
Lateral patellar dislocation
- Tibia fixed, internal femoral rotation and quadriceps contraction.
- Lateral and transient dislocation of the patella.
- The medial patellar facet impacts against the lateral femoral condyle.
- Edema in the bone marrow: inferomedial patella and anterior aspect of the lateral femoral condyle.
- Associated lesions: disruption of the medial retinaculum.

4-Stress Fractures
- At the knee level, it most frequently affects the tibia (middle third).
- Sports: Marathoners, Volleyball.
- Localized pain.
- Start associated with an abrupt change in training.
- They usually respond well to a break from activity for between 4 and 8 weeks.
- If training is not stopped in time, it can develop into acute transverse fractures.
- RX: Cortical radiolucent line without periosteal reaction, 70% of initial X-rays negative, 2 to 6 weeks or months to show alterations.
- MRI: Low-intensity lines in trabecular bone associated with bone edema.


5-Osteoarthritis
- Cartilage degeneration.
- Osteophytes.
- Geodes.
Bone edema in osteoarthritis is strongly associated with PAIN and PROGRESSION of the disease.
Definitive diagnosis:
TRANSIENT BONE MARROW EDEMA vs. OSTEONECROSIS
(To be assessed over time)
Literature
- Lecouvet, Early Irreversible Osteonecrosis Versus Transient Lesions of the Femoral Condyles: Prognostic Value of Subchondral Bone and Marrow Changes on MR Imaging AJR 1998;170:71-77
- Major ;Helms, MR Imaging of the Knee: Findings in Asymptomatic Collegiate Basketball Players AJR 2002;179:641–644
- Hayes ,MR Imaging of Bone Marrow Edema Pattern: Transient Osteoporosis, Transient Bone Marrow Edema Syndrome, or Osteonecrosis RadloGraphics 1993; 13:1001-1011
- Rubin Treatable Chondral Injuries in the Knee: Frequency of Associated Focal Subchondral Edema AJR 2000;174:1099–1106
- Felson, Bone marrow edema and its relationship to progression of knee osteoarthritis. Ann Intern Med. 2003 Sep 2;139(5):330-6.
- Felson et al. The association of bone marrow lesions with pain in knee osteoarthritis. Ann Intern Med. 2001 Apr 3;134(7):541-9
- Pessis E et al. Assessment of progression in knee osteoarthritis: results of a 1-year study comparing arthroscopy and MRI. Osteoarthritis and Cartilage 2003;11:361-69.
- Michael A. Mont, David R. Marker, Michael G. Zywiel, John A. Carrino. Osteonecrosis of the Knee and Related Conditions. J Am Acad Orthop Surg 2011;19:482-494
Some images and graphics were taken from the articles mentioned in the bibliography list.
For any comments or suggestions: radiologyzones@gmail.com
This material was automatically translated from medicosradiologos.com.ar